
Background
According to studies by the WHO, depression is one of the most common mental illnesses worldwide, with a lifetime prevalence of 17% [1] and a 12-month prevalence of 3.2% [2]: this means that more than one in ten people will suffer from at least one depressive episode during their lifetime [3, 4]. Moreover, according to WHO estimates, depression will be the most common disease in industrialized nations by 2030 [5, 6].
Despite existing effective therapeutic approaches such as psychotherapy and medication, only about one third of those currently suffering from depression in Germany receive adequate treatment [7]. Reasons for this include high barriers to seeking professional support, such as the stigma associated with mental illness in our society [8], but also the long wait times to access psychotherapy. This highlights the need for testing and research into new, effective, attractive, and low-threshold therapy services to reduce barriers to uptake and thus steadily improve care for people with depression.
Although studies have shown that physical activity is just as effective in treating depression as psychotherapy or medication with antidepressants, there are currently hardly any formal offers for this in the outpatient sector. Yet physical activity has positive effects not only on the psyche, but also on a variety of physical problems. It also has the potential to be a lower-threshold and less stigmatizing treatment approach than conducting psychotherapy or taking medication. Mindfulness-based practices, as well as relaxation techniques, have also been shown to be effective in the treatment of depression and are recommended as complementary forms of therapy.
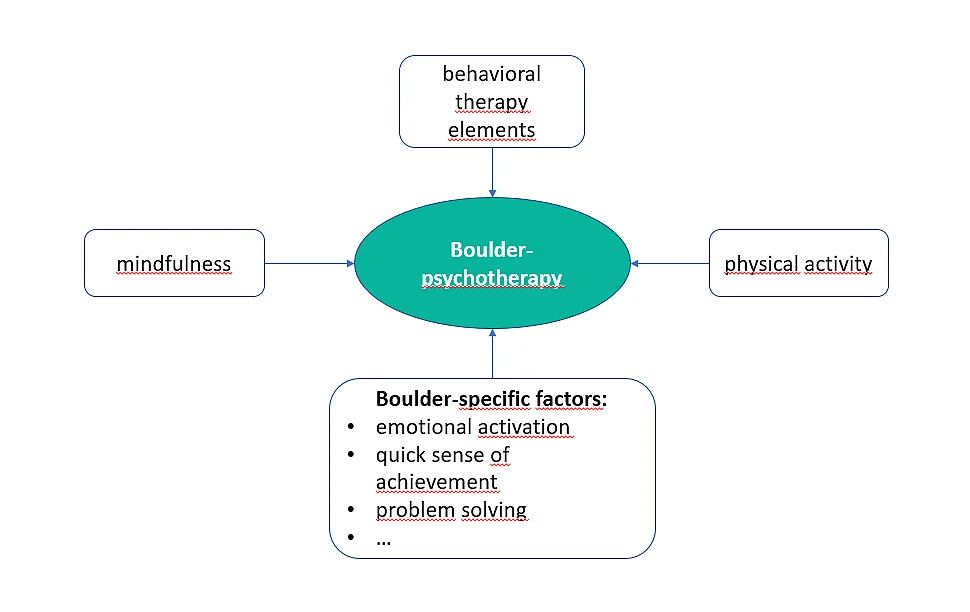
The novel treatment method of combining bouldering and psychotherapy (BPT) is an approach that marries action-oriented elements of bouldering (as a form of physical activity) with psychotherapeutic interventions from cognitive behavioral therapy and mindfulness as well as relaxation exercises.
It thus combines, with the exception of medication, all the therapeutic components that are effective in the treatment of depression and offers access via an attractive type of sport. Climbing, and bouldering in particular, has been growing in popularity in recent years. Initial research results also indicate that climbing and bouldering have specific positive effects on various health areas [9, 10].
Also - but not only - patients with aversions to conventional therapy methods or negative previous experiences with them are facilitated access to psychotherapeutic care through the sport therapy component. In our experience, bouldering together encourages participants to network after the completion of group therapy in order to maintain their newly acquired hobby.
Literature
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Archives of general psychiatry. 1994;51(1):8-19. Epub 1994/01/01.
- Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B. Depression, chronic diseases, and decrements in health: results from the World Health Surveys. Lancet. 2007;370(9590):851-8. Epub 2007/09/11. doi: 10.1016/S0140-6736(07)61415-9.
- Jacobi F, Wittchen H-U, Holting C, Hofler M, Pfister H, Muller N, et al. Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychol Med. 2004;34(4):597-611. Epub 2004/04/22. doi: 10.1017/s0033291703001399.
- Busch MA, Maske UE, Ryl L, Schlack R, Hapke U. Prävalenz von depressiver Symptomatik und diagnostizierter Depression bei Erwachsenen in Deutschland. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. 2013;56(5):733-9. doi: 10.1007/s00103-013-1688-3.
- World Health Organization. The International Classification of Functioning, Disability and Health: ICF. Geneva: World Health Organization; 2001.
- World Health Organization. Global Burden of Disease. 2004 update Genf: World Health Organization, 2008.
- Thornicroft G, Chatterji S, Evans-Lacko S, Gruber M, Sampson N, Aguilar-Gaxiola S, et al. Undertreatment of people with major depressive disorder in 21 countries. Br J Psychiatry. 2017;210(2):119-24. doi: 10.1192/bjp.bp.116.188078.
- Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. Psychological Science in the Public Interest. 2014;15(2):37-70.
- Buechter RB, Fechtelpeter D. Climbing for preventing and treating health problems: A systematic review of randomized controlled trials. Ger Med Sci. 2011;9. Epub 2011/08/25. doi: 10.3205/000142.
- Fruhauf A, Sevecke K, Kopp M. Ist-Stand der Fachliteratur zu Effekten des therapeutischen Kletterns auf die psychische Gesundheit – Fazit: viel zu tun [Current state of the scientific literature on effects of therapeutic climbing on mental health - conclusion: a lot to do]. Neuropsychiatrie. 2019;33(1):1-7. Epub 2018/08/22. doi: 10.1007/s40211-018-0283-0.
KuS pilot study
For the pilot study, a manual for bouldertherapy was developed, which is also currently performed in the regular care of the University Hospital Erlangen (KuS-Therapy www.kletternundstimmung.de).
In the pilot study, over 100 participants were randomly assigned to two groups: either the immediate intervention group or a waiting group. Participants in the intervention group met once a week for three hours at the bouldering gym for a period of eight weeks to conduct bouldertherapy together with two therapists (health care and nursing staff). The waiting group received the regular treatment during this time and were not allowed to participate in a bouldering group until the eight-week intervention phase was completed. All participants were examined five times: once before the start of the intervention phase as a reference value, once immediately after the intervention phase, then at eight weeks, four months, and ten months after the intervention phase. Among other things, they used the Becks' Depression Inventory (BDI) to indicate the extent of their depressive symptoms. The BDI is a self-assessment procedure and contains 21 statements on specific depressive symptoms in the last two weeks, the presence of which the participants can assess.
The BDI assessments showed that the bouldertherapy had a significant positive influence on the depressiveness of the participants. Specifically, the participants in the bouldertherapy group improved on average by one degree of severity from a moderate to a mild depressive symptomatology. These improvements remained stable eight weeks (Luttenberger et al. 2015) or even ten months after the end of the intervention (Schwarz et al. 2019) (see Figure). In addition, positive effects were shown on a number of other domains, such as anxiety, quality of life, and social behavior (Luttenberger et al. 2015). The positive effect of bouldertherapy on depressive symptoms was maintained even when other factors that might affect depressive symptoms (such as additional psychotherapy received, antidepressant use, and participants' general level of physical activity) were controlled for (Stelzer et al. 2018).
Literature
- Schwarz L, Dorscht L, Book S, Stelzer EM, Kornhuber J, Luttenberger K. Long-term effects of bouldering psychotherapy on depression: benefits can be maintained across a 12-month follow-up. Heliyon. 2019;5(12):e02929. Epub 2019/12/25. doi: 10.1016/j.heliyon.2019.e02929. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6911955/
- Luttenberger K, Stelzer EM, Forst S, Schopper M, Kornhuber J, Book S. Indoor rock climbing (bouldering) as a new treatment for depression: study design of a waitlist-controlled randomized group pilot study and the first results. BMC Psychiatry. 2015;15:201. doi: 10.1186/s12888-015-0585-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4548691/
- Stelzer E-M, Book S, Graessel E, Hofner B, Kornhuber J, Luttenberger K. Bouldering psychotherapy reduces depressive symptoms even when general physical activity is controlled for: A randomized controlled trial. Heliyon. 2018;4(3):e00580. doi: 10.1016/j.heliyon.2018.e00580. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5968135/
KuS study
In the KuS study, the manual of bouldertherapy was developed further: it was extended from eight therapy hours to ten, psychotherapeutic contents were added, as well as additional mindfulness and relaxation exercises. With this, Bouldering Psychotherapy (BPT) was born!
Scientific testing of Bouldering Psychotherapy took place in a study across several institutes in several German cities (Dorscht et al. 2019). In this scientific testing Bouldering Psychotherapy was compared with services offered in mainstream care. 233 patients were randomly assigned one of the following interventions: Bouldering Psychotherapy (BPT), cognitive behavioral therapy (CBT) (both in groups), or an activating exercise program. The latter consisted of a home-based, guided exercise program that used similar muscle groups as bouldering psychotherapy. Participants were assessed once before therapy, once immediately after therapy, and three more times up to one year after the end of therapy. The assessment of depressive symptomatology was externally assessed by trained raters during a diagnostic interview (MADRS, Montgomery and Asberg Depression Scale). This was done because external assessments are considered less susceptible to bias than self-assessments.
The BPT group showed a significant reduction in depressive symptoms, from moderate to mild depression symptoms in the external assessment (see figure). These improvements were significantly greater than in the group that had exercised at home with the activating exercise program (Karg et al. 2020). Thus, the effects of Bouldering Psychotherapy were shown to extend beyond those of physical activation alone. As expected, participants in the CBT group also showed significant improvements in depressive symptomatology, although these did not exceed the effects of the BPT group (non-inferiority of BPT compared to CBT). Thus, the hypothesis could be confirmed that Bouldering Psychotherapy is at least as effective as cognitive behavioral therapy, the previous gold standard in depression treatment (Luttenberger et al. 2021).
Bouldering Psychotherapy also showed significant improvements in other areas, such as self-efficacy (Kratzer et al. 2021). Furthermore, despite its somewhat higher costs due to facility admissions, Bouldering Psychotherapy was assessed as a cost-effective type of depression treatment in a health economic evaluation (Schwarzkopf et al. 2021).
Literature
- Dorscht L, Karg N, Book S, Graessel E, Kornhuber J, Luttenberger K. A German climbing study on depression: a bouldering psychotherapeutic group intervention in outpatients compared with state-of-the-art cognitive behavioural group therapy and physical activation - study protocol for a multicentre randomised controlled trial. BMC Psychiatry. 2019;19(1):154. Epub 2019/05/19. doi: 10.1186/s12888-019-2140-5.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6525374/ - Karg N, Dorscht L, Kornhuber J, Luttenberger K. Bouldering psychotherapy is more effective in the treatment of depression than physical exercise alone: results of a multicentre randomised controlled intervention study. BMC Psychiatry. 2020;20(1):116. Epub 2020/03/14. doi: 10.1186/s12888-020-02518-y.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7066840/ - Luttenberger K, Karg-Hefner N, Berking M, Kind L, Weiss M, Kornhuber J, Dorscht L. Bouldering psychotherapy is not inferior to cognitive behavioural therapy in the group treatment of depression: A randomized controlled trial. Br J Clin Psychol. 2021 Nov 17. doi: 10.1111/bjc.12347.
Bouldering psychotherapy is not inferior to cognitive behavioural therapy in the group treatment of depression: A randomized controlled trial - PubMed (nih.gov) - Kratzer A, Luttenberger K, Karg-Hefner N, Weiss M, Dorscht L. Bouldering psychotherapy is effective in enhancing perceived self-efficacy in people with depression: results from a multicenter randomized controlled trial. BMC Psychol. 2021 Aug 26;9(1):126. doi: 10.1186/s40359-021-00627-1. PMID: 34446114; PMCID: PMC8393466.
Bouldering psychotherapy is effective in enhancing perceived self-efficacy in people with depression: results from a multicenter randomized controlled trial - PubMed (nih.gov) - Schwarzkopf L, Dorscht L, Kraus L, Luttenberger K. Is bouldering-psychotherapy a cost-effective way to treat depression when compared to group cognitive behavioral therapy - results from a randomized controlled trial. BMC Health Serv Res. 2021 Oct 26;21(1):1162. doi: 10.1186/s12913-021-07153-1
Is bouldering-psychotherapy a cost-effective way to treat depression when compared to group cognitive behavioral therapy - results from a randomized controlled trial - PubMed (nih.gov)
